A 19years old female with complaints of cough with sputum
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent.
Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 19 year old girl studying 12th grade from devarakonda came to the GM OPD with
CHIEF COMPLAINTS -
Cough with sputum from 5 days.
HOPI :
Then she developed fever which was insidious in onset , gradually progressive , high grade , continuous , not associated with chills and rigors , No evening rise of temperature, no Sweating , relieved on medication.
No H/O SOB , chest pain, chest tightness , loss of appetite , weight loss , palpitation, burning micturition, Wheeze present.
Past history :
Similar complaints of fever with cough and sputum 1 year ago ( about one week)
● H / O SOB on exertion , relieved on rest
● No orthopnea , PND
● H /O Hospital admission for this.
● No H/O inhaler usage
● No H/O TB, DM, HTN, CAD, epilepsy , thyroid
Family history:
Her sister had difficulty in breathing
Her sister died in the past after intake of poison
Social history:
She wakes up at 6am
Goes to college at 9:30
She will have lunch at 1pm
Comes home by 5:30pm
Studies for 1-2 hours
Has dinner at 9pm
Goes to bed at 10 pm
This routine has changed due to her health issues
Personal History -
She consumes mixed diet with normal appetite
She has adequate sleep
Her bowel and bladder movements are regular
She has no Allergies and Addictions.
General Examination :
Patient is conscious, coherent, cooperative.
Temperature - 98.6°F
Pulse - 86 beats/min
BP - 100/60 mmHg
RR - 18 cycles/min
GRBS - 107 mg/dl
SPO2 - 98 %
Pallor present
No Icterus ,Clubbing ,Cyanosis, Lymphadenopathy
SYSTEMIC EXAMINATION :
CVS :
S1,S2 heard
No thrills ,murmurs
RESPIRATORY SYSTEM :
URT:
Nose: Left DNS present,No nasal polyps
Oral cavity : Normal oral hygeine
Posterior pharyngeal wall = Normal
LRT:
INSPECTION:
Shape of chest : Elliptical, B/L Symmetrical
Trachea : Appears to be central
Chest movements : equal on both sides
Apical Impulse : not seen
No supraclavicular and infraclavicular hollowness
No crowding of ribs , drooping of shoulders , Wasting of muscles.
No usage of accessory muscles of respiration
No Kyphosis, Scoliosis , Sinuses , Scars , Engorged Veins and visible pulsations.
PALPATION:
No local rise of temperature
No tenderness
All inspectory findings are confirmed
Trachea : central
Chest movements : equal on both sides
Apex beat : Felt at 5th ICS medical to MCL
TVF : Increase in Rt ISA, Infra SA,IAA
AP diameter -20 cm
Traverse - 25cm
Right Hemithorax - 37cm
Left thorax - 36 cm
Chest circumference -
Inspiration - 75cm
Expiration - 73cm
Chest expansion - 2cm
Vocal fremitus equal on both sides in all areas
PERCUSSION -
Resonant in all areas on both sides
AUSCULTATION -
BAE +ve
NVBS
Crepitus is heard in Right suprascapular, infrascapular, infraclavicular and left infraclavicular, infrascapular.
Vocal resonance same on both sides
ABDOMEN :
Shape - Scaphoid
No tenderness, palpable mass, No Fluid
No bruits
Liver not palpable
Spleen not palpable
No Bowel sounds
CNS Examination
Pt is Conscious ,coherent, cooperative
Speech normal
Cranial nerves, motor system, sensory system Normal
INVESTIGATIONS:

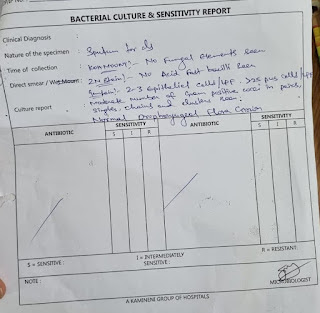

PROVISIONAL DIAGNOSIS:
Bronchiectasis
TREATMENT :
Inj PIPTAZ 4.5gm IV TID
Inj PAN 40 mg IV OD BBF
Syp ASCORIL 2tsp TID
Neb with Ipravent 6th hourly
- Budecort 8th hourly
Tab MUCINAC
Tab PCM High protein diet
IVF NS @75 ml/hr
Monitoring vitals
Chest physiotherapy


Comments
Post a Comment